Promoting mental health through clinical psychotherapy and counseling, creative art therapy and art open studios, education and training, clinical supervision, and consultation.
Author: percepta therapeutic
PerceptA Therapeutic and Training Center, LLC is located in Baltimore, Maryland, and provides individual and group psychotherapy, and counseling, art as therapy, training, supervision, and consultation services.
Dr. Chioma Anah, Ed.D., ATR, NCC, LCPC, ACS
is a Registered Art Therapist, National Certified Counselor,
Licensed Clinical Professional Counselor (Maryland),
Approved Clinical Supervisor, and Founder & CEO of PerceptA
Therapeutic and Training Center, LLC in Baltimore, Maryland.
She has over 15 years experience in the clinical field working
with adults, adolescents and children, and is a
Board Approved Supervisor in Clinical Professional Counseling.
In keeping with our Counseling Awareness Month theme, particularly, our ongoing effort to educate the public about several areas of professional counseling, and the contributions of professional counselors nationwide; today, it is with the greatest honor and privilege that I introduce to you, Michelle E. Wade, Ed.D., LCPC, LPC, NCC, ACS. Please join me in welcoming her, as she guest posts for us today.
If you are a member of the American Counseling Association (ACA), then Dr. Wade is no stranger to you. Dr. Wade is an active member of the ACA, and has contributed immensely, in many ways, to the field of professional counseling and counselor education.
Dr. Wade has a Doctorate of Education in Counselor Education and Supervision (Ed.D); is a Licensed Clinical Professional Counselor (LCPC-Maryland); a Licensed Professional Counselor (LPC-VA); a Nationally Certified Counselor (NCC); and an Approved Clinical Supervisor (ACS).
Today, Dr. Wade shares her expertise about The Future of Counseling, particularly the role of technology in counseling:
Counseling 2.0 – The Future of Counseling
By Michelle E. Wade, Ed.D., L.C.P.C., L.P.C., N.C.C., A.C.S.
The American Counseling Association (ACA) (Kaplan, Tarvydas, & Gladding, 2013) defines counseling as “a professional relationship that empowers diverse individuals, families, and groups to accomplish mental health, wellness, education, and career goals” (p. 2). In the 21st century, the way that professional relationship is established is no longer necessarily depicted as a client in the opposite chair from the counselor. Rather, counseling can now be conducted over vast distances and the counselor-client relationship can be developed and maintained outside of the therapy room.
Counselors are taught from the very beginning of training that the therapeutic relationship between counselor and client is paramount and as such the relationship needs to be developed and nurtured (Wampold, Duncan, & Miller, 2009). Lambert and Barley (2001) report that thirty percent (30%) of beneficial counseling outcomes can be attributed to the professional relationship. Fluckiger, Del Re, Wampold, Symonds, and Horvath (2011) explicate the alliance-outcome relationship has a greater correlational link greater than any other treatment variable studied. Therefore, if the relationship is paramount, one has to ask whether counseling should venture into this brave new frontier with clients.
***Dr. Michelle E. Wade is an ethics specialist with ACA Ethics Department, and serves as co-editor of the ethics inquiries column for the ACA publication, Counseling Today. For ACA members with questions about ethics, please submit questions or comments to mwade@counseling.org with subject line “Ethics Column.” Dr. Wade can also be reached via Email- UltreyaTherapy2005@gmail.com
If you are interested in writing a guest post, please send submissions to Dr. Chioma Anah – Email- dr.c.anah@gmail.com
20/20 Definition of Counseling– “Counseling is a professional relationship that empowers diverse individuals, families and groups to accomplish mental health, wellness, education and career goals.”
April is Counseling Awareness Month- an opportunity to educate the public about the counseling profession, as well as its positive impact on society, both locally and globally.
Just last month, I had the opportunity to attend the ACA 2015 Conference & Expo in Orlando, Florida; a transformative experience, with many new lessons learned, and old ones reaffirmed.
Counselors are incredible individuals who; hold and honor the stories of their clients in an empathic and respectful way. They help prompt/promote change and healing for their clients that lasts a lifetime (Kottler & Balkin -Keynote Speakers- ACA 2015 Conference & Expo). Counselors do good and very important work every day, and contribute to communities nationwide. Mariel Hemingway (Keynote Speaker @ACAOrlando2015) said it best, when she said, “What you do, is so important.”
To kick start this month properly, here are 12 Things that you should know about Professional Counselors- by Morgan Spurlock- Keynote Speaker, 2014 ACA Conference & Expo:
12 Things About Professional Counselors
Counselors have a graduate degree or higher in counseling.
Counselors emphasize multicultural competence and respect for diverse worldviews.
Counselors focus on wellness, career development, and client empowerment as opposed to psychopathology- a proactive approach to mental health.
Counselors encourage people to be genuine and to work to find their own authentic self, even if the authentic self is somewhat different from dominant culture norms.
Counselors assist issues caused by typical life stressors, such as grief and loss, relationship problems, and developmental challenges throughout the lifespan.
Counselors diagnose/or treat mental disorders.
Counselors are often trained in reacting to disasters- those created by individuals and nature.
Counselors serve as a front line resource in schools, as the eyes and ears for early signs of emotional distress caused by bullying, harassment, and other forms of abuse and trauma.
Counselors play an important role on college campuses, as the number of students visiting counseling centers is steadily increasing.
Counselors work with military veterans to help them with depression, PTSD, the transition back into civilian life, and more.
Counselors abide by ACA’s Code of Ethics. aca-code-of-ethics– The 2014 ACA Code of Ethics replaces the 2005 edition. It’s the First code that speaks to the ethics of using social media with clients.
Counselors are passionate, diverse, and committed to helping people from all walks of life and all depts. of despair to survive as thrive in today’s world.
I have been a professional counselor for 15 years, and remain very committed to spreading the word about professional counseling, and the awesome work counselors around the nation do every day.
Keep an eye on this site throughout the month of April, as I share with you all, the extraordinary work counselors have done, and continue to do, today.
Also, please feel free to share with us some of the wonderful work you are doing as professional counselors.
I had the pleasure of attending the ACA 2015 Conference & Expo from March 12-15 in Orlando, Florida. What an awesome and inspirational experience! Here are some of the highlights:
The Conference was held at the beautiful Hyatt Regency Hotel, Orlando, and what a gorgeous hotel it was, filled with incredible artwork:
Guy Dill “Roscoe” 2009 AluminumJim De France Custom Commission Mixed Media on WoodRobert Walker Untitled, 1986 Mixed Media
Keynote Speakers:
Mariel Hemingway- Friday, March 13th
Dr. Richard Balkin and Dr. Jeffrey Kottler- Saturday, March 14th.
Actress, Mariel Hemingway- About counselors…”You create a safe space for people to find themselves.”
Mariel Hemingway- Friday, March 13, 2015 ACA Conferences 2015
Dr. Richard Balkin and Dr. Jeffrey Kottler- The Power of Relational Connection! “Counseling is a professional relationship…counseling promotes wellness…stories are what creates relationships.”
Dr. Jeffrey Kottler and Dr. Richard Balkin
“100% of what we do in counseling is holding and honoring [the stories of our clients] and helping them see a different path…and promote change that lasts a lifetime”- Kotter, ACA Conference 2015
Dr. Kottler & Dr. Balkin
Education Sessions
Friday, March 13, 2015
Kara Lauren Carnes-Holt, Kristen K. Meany-Walen, Andy Felton-Express Yourself: Creative Strategies for Counseling Supervision
Dr. Gerald Corey & Dr. Jamie Bludworth- Becoming a Professional Counselor. “As counselors, self-care is our responsibility…take responsibility for your own self-care.”
Dr. Michelle A. Mitcham, Dr. Beverly J. O’Bryant, Dr. Cirecie West-Olatunji, Dr. Angela D. Coker, Dr. Rhonda M. Bryant, Dr. Cheryl Holcomb-McCoy, Dr. Tarrell Awe Agatha Portman, Dr. Wendy Greenidge, and Dr. Norma L. Day-Vines- Courageous Conversations with Women of Color in Counselor Education: Surviving and Thriving.
“Stay focused…your work will speak for itself.”- Dr. Day-Vines, 2015 ACA Conference
Education Sessions
Saturday, March 14, 2015
Dr. Justin D. Lauka- A Social Justice Approach to Cognitive Behavioral Therapy. “Social Justice- is a process of acknowledging systemic societal inequalities and oppression while acting responsibly to eliminate the systemic oppression in the forms of racism, sexism, heterosexism, classism, and other biases in clinical practice both individual and distributive levels” (Odegard & Vereen, 2010, p. 130).
Dr. David Kaplan and Art Terrazas- Keeping Up with the Counseling Profession: Current Issues on the National Level
Dr. David Kaplan
Dr. Courtland Lee, Dr. Vivian Lee, & Dr. Dione Mifsud- Counselors as Global Citizens: Developing Transcultural Counseling Competency
Dr. Courtland Lee-Transcultural Counseling Competency
“Transculturally competent counselors are globally literate human beings who view themselves as global citizens who can think and act locally and globally” (Courtland Lee, ACA 2015 Conference).
Dr. Derald Wing Sue- Microaggressions in Everyday Life: Implications for Mental Health Practice
Racial Microaggressions- Dr. Derald Wing Sue
“Microaggressions are constant and continual without an end date” (Derald Wing Sue, ACA 2015 Conference).
More pictures from the conference:
New ACA President- Dr. Thelma Duffey
Mariel Hemingway
I’m a Counselor, What’s Your Superpower?
Robert L. Smith, Ph.D., NCC- ACA President
Garry R. Walz Trailblazer Award
ACA Opening Night Celebration- Friday, March 13, 2015
The 2016 ACA Conference will be in Montreal, Canada from March 31, 2016, to April 3, 2016. See you there!
American Harvard Psychiatrist, Chester Middlebrook Pierce first coined the term racial microaggression in the 1970s to refer to automatic and often subtle “put downs” directed toward African Americans (Dr. Pierce is currently Emeritus Professor of Education and Psychiatry at Harvard Medical School). In 2007, Columbia professor Derald Wing Sue, who is recognized as one of the most influential scholars focusing on the study of racial microaggressions, expanded on the work of Pierce and colleagues, and proposed a conceptual framework of how racial microaggressions manifest in the everyday lives of people of color. Dr. Sue defined racial microaggressions as, “Brief and commonplace daily verbal, behavioral, and environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults to the target person or group.”
Key points about Racial Microaggressions:
a) It is not the “old fashioned” Jim Crow type of racism that is most hurtful to Black Americans, but the new contemporary and subtle forms of racism known as racial microaggressions. Despite the election and re-election of an African American male president, we are not living in a “post-racial” era.
In 2010, it was estimated that, 68% of African Americans were dissatisfied and reported inequalities and racism in their daily lives- while 71% of Whites reported satisfaction with the way racial relations was.
These percentages might be different today in 2015, given all the racial unrest following the Trayvon Martin, Michael Brown, and Eric Garner tragedies. It is hard to forget the images of protests and riots in Ferguson, Missouri, and subsequently, in many other cities around the United States.
b) They are subtle, insensitive, automatic and sometimes unconscious verbal, non-verbal, and/or visual insults and indignities directed towards Black American people or people of color.
c) They are quick, everyday interactions that send hurtful, denigrating messages to Black Americans and other people of color that implies that: * they do not matter;*they are not valued or respected; *they are lazy; they are unintelligent; *they are invisible; *they are always aggressive and angry; *they are criminals and should be feared at all times; *they are dangerous and a threat to society; *they are sub-human and demon-like; *they are all the same; and that *they are second-class citizens.
e) Racial microaggression can be invisible, often overlooked, and sometimes unconscious. However, they can be very damaging, and could create lethal consequences for the recipient. The most lethal and extreme example of the consequences of racial microaggressions, came in the case of Officer Darren Wilson and his reaction when he saw Michael Brown:
29-year old White Officer, Darren Wilson, shot and killed 18-year old Michael Brown on August 9, 2014. This is what Officer Wilson saw, the day he shot Michael Brown- in his words: “I felt like a five-year old holding onto Hulk Hogan…Hulk Hogan, that’s just how big he felt and how small i felt just from grasping his arm…The only way I can describe it, it looks like a demon, that’s how angry he looked. He comes back towards me again with his hands up…At this point it looked like he was almost bulking up to run through the shots, like it was making him mad that I’m shooting at him. And then when it [the bullet] went into him, the demeanor on his face went blank, the aggression was gone, it was gone, I mean I knew he stopped, the threat was stopped.
f) Perpetrators of racial microaggression are often well-intentioned Whites in American society who are unaware of the highly charged racial situations. They are often the product of America’s complicated history with race and still harbor racial biases and display discriminatory behaviors towards Black Americans in all areas of society, including education and employment.
g) Racial microaggressions could be challenging for all involved because of the clash of racial realities; the racial reality of Black Americans is different from that of White Americans. In some cases, when the victim confronts the perpetrator about the racial microaggressions that they have just experienced, the perpetrator’s responses run the gamut from, pointing out that he or she only meant the slights as a compliment, to claiming that the comment was merely a joke. Further, the perpetrator sometimes accuses the recipient of being too sensitive when they are offended by the comment or action.
h) Many of the perpetrators of racial microaggressions blame the victim…”If only Black people worked harder, they would be successful,” or, “Not everything is about race.”
i) Racial microaggressions create psychological harm for Black Americans manifested in symptoms that include, depression, paranoia, anxiety and PTSD.
j) Racial microaggressions create physiological harm for Black Americans. According to Adewale Troutman, MD, Director, Louisville, KY Department of Public Health & Wellness, and S. Leonard Syme, Professor of Epidemiology, UC Berkeley, there are significant effects of racism on the health outcomes of people of color. Through research, Dr. Troutman suggests that, “If you are African American, no matter your social status; your health outcomes are going to be worse than that of your White counterpart.” He goes on to state that African American’s die earlier than Whites and have higher rates of medical diseases such as diabetes, hypertension, high blood pressure, and coronary artery disease. Dr. Syme adds that, “Hyper vigilance and the burden of constantly being on guard (as a Black American) over time, changes biological markers that make people vulnerable to getting sick.”
k) Racial microaggression is often downplayed, ignored and/or dismissed as a legitimate issue, and many White Americans question the existence of racial prejudice and discrimination, particularly when the country elected a Black President twice in a row.
16 examples of Racial Microaggressions (These are examples of actual experiences of many Black Americans):
1) “You should be proud of yourself. You are not like the rest of them; you are a credit to your race.”
2) “You sounded so different on the phone; you were not what I expected.”
3) “Sorry, I thought you were the nurse, not the doctor.”
4) “You guys must be really happy now that Obama is president, there should be no more excuses or complaints from you people.”
5) “I’m surprised you haven’t seen, ’12 Years A Slave’ yet, I though you would be one of the first people to go watch it.”
6) “You are so exotic looking. What are you?”
7) “That was really a great class, Dr. Smith, but next week, you may want to think about doing a role-play to demonstrate your examples because I learn better that way as a student…I’m just saying.”
8) “Hey, I’ve been stopped by cops before, just driving and I didn’t make a capital case about it. Not everything is about race.”
9) “Why does every Black person pull the race card whenever they are backed into a wall? Many of the seemly racially motivated bad experiences they have experienced, I’ve experienced some of them as well, and besides, if it quacks like a duck and walks like a duck, well, it’s a duck!”
10) “People are people. I really don’t see race or color in this situation.”
11) “Do you think your stress is from something else instead of your everyday racial experiences?”
12) “The President of the United States is Black. I really don’t see where all this racial angst is coming from. Why are you people still so angry?”
13) “How do Black people feel about…?” (Fill the blank with every issue relating to Black society- as if they are the spokesperson for all issues concerning Blacks in society).
How do Black people feel about Obama, now that he’s not so popular?
How do Black people feel about Tiger Woods…?
And the list goes on…
14) “Wow, you listen to Radiohead, and you actually know who Beck is? I though Kanya West and Jay-z would be more your speed.”
15) “You have a nice home, you drive a nice car, and you are living the ‘American Dream’ what else do you have to complain about? You are doing better than most Whites…but you always complain about your poor treatment because of your race. Look at everything that you have…what is the problem?”
16) “I have lots of Black friends, I am not racist!”
President Obama’s experiences of Racial Microaggressions:
Following the acquittal of George Zimmerman in the Trayvon Martin case, President Obama gave a speech to the public. Although he did not mention it by name, many of the experiences President Obama describes here are racial microaggressions:
“Trayvon Martin could have been me 35 years ago…I think it’s important to recognize that the African American community is looking at this issue through a set of experiences and a history that doesn’t go away…There are very few African American men who have not had the experience of being followed when they were shopping in the department store. That includes me. And there are very few African American men who haven’t had the experience of walking across the street and hearing the locks click on the doors of cars. It happens to me, at least before I was a senator. There are very few African Americans who haven’t had the experience of getting on the elevator and a woman clutching her purse nervously and holding her breath until she had a chance to get off. That happens often” (Obama, 7/19/ 2013).
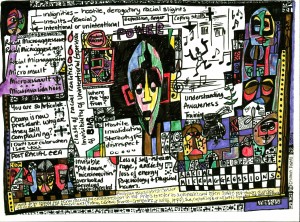
“Artists are the gatekeepers of truth. We are civilization’s radical voice.” – Paul Robeson
“Racial Microaggressions: Everyday experiences of Black men”- Mixed Media- 2014 by Chioma AnahRacial Microaggressions- 2015 by Chioma Anah – 2/2015
What can be done about Racial Microaggressions?
a) Recognizing and acknowledging our difficult history with race in the United States, and acknowledging and confronting our own cultural biases, assumptions and worldview.
b) Understanding that race matters in the United States, and that racism and injustice hurts ALL of us.
Increasing our awareness about issues of race and diversity in the United States.
Using our understanding of diversity and race in a way that connects all of us with the common goal of creating a more socially just environment.
c) Improving our education and training surrounding cultural sensitivity in an effort to combat acts of microaggression.
d) Engaging in Appropriate Planning & Action about racial microaggression, which includes facilitating and encouraging open and honest discussion on the subject of race, culture and microaggressions with different races. Again, the goal here is to create awareness, understanding, healing, and appropriate action, leading to a more socially just and culturally sensitive nation.
***Have you experienced Racial Microaggressions? Do you recognize yourself in this post as the perpetrator or the victim of racial microaggressions?
What are the best ways to respond to racial microaggressions when they occur?
How can an awareness of racial microaggression inform society around the issue of diversity?
What do you think can be done about combating racial microaggressions in society?
We would like to hear from you.
Chioma Anah, EdD, ATR, NCC, LCPC, ACS
Brief Bio: Dr. Chioma Anah has a doctorate in Counseling Psychology, is a Registered Art Therapist (ATR), National Certified Counselor (NCC), Licensed Clinical Professional Counselor (LCPC- Maryland), Approved Clinical Supervisor (ACS), and Founder, CEO, & Director of PerceptA Therapeutic and Training Center, LLC. She has over 15 years experience in the clinical field working with at-risk adolescents, adults and families of all races and cultural background. Dr. Anah’s research interest includes multicultural issues in counseling; specializing in racial microaggressions in everyday life and implications for clinical practice. Dr. Anah is committed to highlighting the impact of racial microaggressions, multicultural issues, and social justice issues, as it relates to diverse clients in therapy.
Contact Dr. Anah regarding this post: Email: dr.c.anah@gmail.com
Our interview series, “PerceptAInterviews” continues. Today, we are so honored and privileged to interview Erica Weinstein, MEd, NCC, LCPC, owner of Weinstein Wellness Mobile Psychotherapy. Thank you Ms. Weinstein, for sharing your thoughts, experiences, and time with us!
Erica Weinstein, MEd, NCC, LCPC
Erica Weinstein, M.Ed., N.C.C., L.C.P.C.
Ms. Weinstein has a Master’s degree from Loyola College in Maryland; she is a Nationally Certified Counselor (NCC), and a Licensed Clinical Professional Counselor (LCPC- Maryland). Ms. Weinstein is a remarkable young woman who owns WEINSTEIN WELLNESS Mobile Psychotherapy, an In-Home & Office Psychotherapy Service, working with individuals, couples and families. Her practice specializes in individuals with a variety of mental health issues, including Anxiety, Trauma, & Mood Related Disorders. Ms. Weinstein, will meet with you, in the comfort & convenience of your home of her office; in essence, she will work with you to arrange a location that works best with you. Ms. Weinstein considers herself a, “Turner of thoughts, challenger of perspectives, and seeker of the new & bright…”
Interview Questions by PerceptA Therapeutic and Training Center, LLC
What drew you to become a counselor and how did you become interested in the professional? Share some of your background.The wonderment of how humans think drove me to become a therapist. I believe I was born to help others search.
Where did you earn your Master’s Degree? What made you pick that school and what was your experience like?I earned my Med in School Counseling from Loyola College in Baltimore MD. Honestly, theirs was the first & only program I considered…felt right at the time. I was thoroughly academically challenged & overwhelmed. Happy I experienced it; overjoyed that it’s completed.
When and why did you choose to go into private practice?Almost 2 years to the day I waded into the shaky waters of private psychotherapy practice. I had spent enough years & energy working as an underling (despite the quality of my education & experience) in the field. It was time to dance my dance, my way.
What are some of your professional challenges in private practice and how do you successfully deal with those challenges?One challenge of operating a private psychotherapy practice is how to go about introducing myself & my services to those who may benefit. I manage this by trying everything even slightly reasonable.
2015 promises to be an innovative, creative, informative, research driven, and inspirational year here at PerceptA Therapeutic and Training Center, LLC. We have many exciting things to look forward to this year:
The ACA Conference in March, and the AATA Conference in July; posts by experts in the field of counseling and psychology; interviews conducted with prominent professionals in the counseling field; supervision resources for counselors, and therapists looking to use art in their work with clients- particularly clients of color; and resources for graduate/doctoral students, especially during the dissertation portion of the process.
We are also interested in research.
What are your contributions in the larger context of the counseling psychology literature? We would like to hear from you! Special attention will be given to multicultural and social justice issues in counseling.
We continue to honor the fact that mental health should be treated and respected, much the same way as other medical issues.
Thank you,
~The PerceptA Team
Please follow us, and continue to include us in your journey:
The tragic death of beloved actor and comedian, Robin Williams (July 21, 1951- August 11, 2014), from an apparent suicide, has put a long overdue national spotlight on mental illness. Following his death, his media representative, released a statement that, in part, read that Williams had been, “battling severe depression of late.”
Authorities believe that the “Awakings,” “Dead Poets Society,” “Good Will Hunting,” “Mrs. Doubtfire,” “Aladdin,”and “Good Morning Vietnam,” genius actor’s ongoing battle with depression and bipolar disorder contributed to his suicide; Williams admittedly, also suffered from drug and alcohol addiction, and recently reports have indicated that he was also going through the early stages of Parkinson’s disease.
Robin Williams 1951-2014
Depression is real. Depression is a devastating and serious illness that should not be taken lightly, and if not professionally treated, can end in life threatening consequences that can include suicide.
In America alone, it is estimated that 7% of the population is suffering from major depressive disorder. In addition, the World Health Organization reports that over 300 million people globally are suffering from this disease. With these staggering numbers, it is time that depression gets brought out of the shadows and into the national conversation, with a focus on education to promote understanding in order to erase the sigma that is so often associated with mental illness. Perhaps more lives can be saved this way.
According to the Diagnostic and Statistical Manual of Mental Disorders- 5th Edition (DSM-5), Major depression is characterized by, “the presence of sad, empty, or irritable mood, accompanied by somatic and cognitive changes that significantly affect the individual’s capacity to function.”
Depressive symptoms include:
Depressed Mood: Sadness, hopelessness, feelings of worthlessness and guilt.
Recurrent thoughts of death or suicidal ideations or suicide plans or attempts.
Changes in appetite, and sleep.
Difficulty thinking, concentrating or making decisions.
Constant fatigue and low energy.
Loss of interest or enjoyment in activities previously seen as pleasurable.
Depressive symptoms can persist every day for at least 2 consecutive weeks, with impairment in social, occupational, and other significant areas of functioning. Also, for a diagnosis to occur, 5 or more of the symptoms highlighted above have to be present those 2 weeks, with depressed mood or loss of interest or pleasure in activities being one of the symptoms.
More information about depression from the National Institute of Mental Health can be seen here:
Bipolar disorder is a mental disorder characterized by shifts in moods from manic to major depressive episodes. It is actually believed that Williams had been diagnosed with Bipolar Disorder.
According to the DSM-5, manic episodes are characterized by:
Decreased need of sleep and increased racing thoughts and/or flight of ideas.
Increased involvement in activities with a high potential of risk and consequences (over spending, risky sexual behaviors, gambling).
Inflated self-confidence and grandiosity.
Increased goal-directed activity and excessive planning of multiple activities.
Pressure to keep talking and distractibility.
The mood in a manic episode is generally described as euphoric and, “feeling on top of the world.”
There is no cure for bipolar disorder; however, it can be treated with ongoing medication and psychotherapy. Some people with bipolar disorder choose not to keep taking the medication prescribed because many describe that the medications typically dulls their senses. For this reason, If you have a loved one suffering from this disease: be loving and supportive, and remember that mental illness is a disease and should be treated in the same way a diagnosis of cancer is handled. They should be encouraged to follow their medication regime as prescribed by their doctor and also, continue to be educated about the illness including treatment options with their doctor.
For those suffering from this illness, we encourage you to please seek professional help and/or contact I-800-273-TALK (8255)
More information about bipolar disorder from the National Institute of Mental Health can be seen here:
The following is the first of a new interview series; “PerceptAInterviews.” PerceptA will be conducting a series of interviews with professionals from a variety of backgrounds, for the benefit of all students in need of guidance regarding their own professional path.
Our first interview is with Dr. Beth Gonzalez-Dolginko.
Dr. Beth Gonzalez-Dolginko
Beth Gonzalez-Dolginko, EdD, LCAT, LP has worked clinically as an art therapist for 40 years, in academia for 28 years and in private practice for 36 years. Beth has worked with children and adults in the areas of psychiatry, addictions, aging, PTSD, chronic illness, special education, developmental disabilities and child development. Beth currently serves on the New York State Office of the Professions for Mental Health Practitioners Board.
1. What drew you to become an art therapist and how did you become interested in the profession? Share some of your background.
When I was a teenager, I was interested in art and psychology, so I used to say I wanted to be an art therapist, even before I actually knew it was a profession. I have been working clinically for 40 years, both in private practice and institutions, in: in-patient psychiatry, with PTSD, with developmental disabilities, with the medically ill, in special education, in child development, with aging and with addictions issues. I have also taught art therapy on both the undergraduate and graduate levels for 28 years.
2. Where did you earn your PhD/EdD? What made you pick that school and what was your experience like.
My EdD is in Foundations, Leadership and Policy Studies in Education Administration. Honestly, I needed only my Master’s in art therapy for my NYS license. I earned a doctorate because I was a professor on a full-time tenure track at Hofstra University and was required to get my doctorate. I earned it at Hofstra because I got tuition remission, and I was right there.
3. What is your area of expertise?
My areas of expertise as both an art therapist and psychoanalyst are psychiatry and child development.
4. How did your education get you where you are now?
Again, I needed only my Master’s in art therapy for my NYS license. My Master’s in Art Therapy, getting my ATR-BC and my license are what has served my professional path.
5. What benefits have you had since earning your PhD?
None, really. I am on a NYS Board for Mental Health Practitioners, and there is some recognition from them but not really in terms of my practice. The knowledge of how to engage in meaningful research and write professionally is probably the best outcome of earning my doctorate.
6. What advice would you give the future generation of art therapists about what is important in the field?
It is important to stay current with trends in the field of psychotherapeutic treatment and engage in research related to these fields. The more research and publications that exist related to art therapy, the more credibility our profession will have. It is also important to work towards licensure in your home state. We finally got it in NYS. It has not necessarily increased our salaries, but it has given us more credibility and visibility.
7. In regards to picking a graduate school and choosing a program to suit their needs, what advice would you give to art therapists?
It is important to do your homework and pick a program that matches your philosophy and personality. Look at where their internship placements are. Definitely, do a face-to-face interview with the program director or other faculty members, and ask plenty of questions. You should interview them, too. The location might be an important consideration, as well.
Please join us in welcoming our new intern, Orly Rosenberg to the PerceptA family. We are very lucky and honored to have Ms. Rosenberg, who will be focusing on Social Media Management, Research, and offering a student perspective on therapeutic issues. Welcome aboard Ms. Rosenberg!